

Automated continuous noninvasive ward monitoring: future directions and challenges
- PMID: 31146792
- PMCID: PMC6543687
- DOI: 10.1186/s13054-019-2485-7
Automated continuous noninvasive ward monitoring: future directions and challenges
Abstract
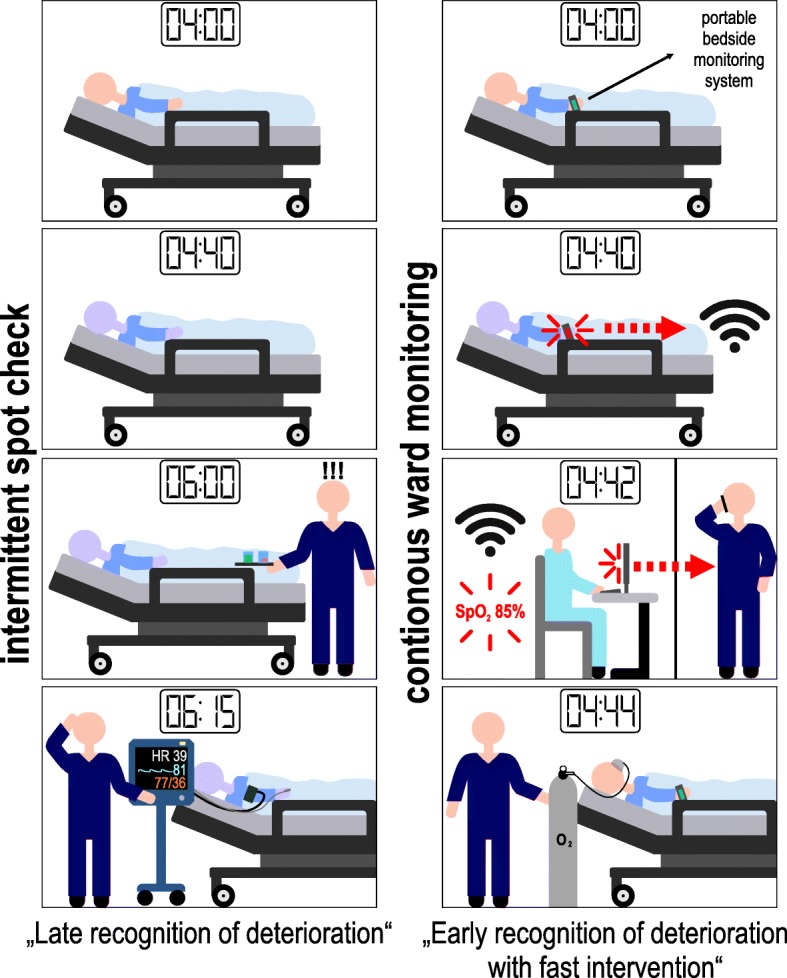
Automated continuous noninvasive ward monitoring may enable subtle changes in vital signs to be recognized. There is already some evidence that automated ward monitoring can improve patient outcome. Before automated continuous noninvasive ward monitoring can be implemented in clinical routine, several challenges and problems need to be considered and resolved; these include the meticulous validation of the monitoring systems with regard to their measurement performance, minimization of artifacts and false alarms, integration and combined analysis of massive amounts of data including various vital signs, and technical problems regarding the connectivity of the systems.
Keywords: Artifacts; Blood pressure; False alarms; Hemodynamic monitoring; Hypotension; Hypoxemia; Normal ward; Peripheral oxygen saturation; Postoperative complications; Remote monitoring.
Conflict of interest statement
AKK collaborates with Medtronic (Boulder, CO, USA) as a member of the executive advisory board on respiratory monitoring and steering committee member of the PRODIGY trial and receives honoraria for these services including giving lectures and refunds of travels expenses. AKK serves on the clinical advisory board for Retia Medical (Valhalla, NY, USA), Linshom Medical (Ellicott City, MD, USA), and also serves as a consultant for La Jolla pharmaceuticals (San Diego, CA, USA) and as a subject matter expert for the development of the Anesthesia SimStat system for CAE healthcare (Sarasota, FL, USA). BS collaborates with Pulsion Medical Systems (Feldkirchen, Germany) as a member of the medical advisory board and received honoraria for giving lectures and refunds of travel expenses from Pulsion Medical Systems. BS received research support and honoraria for giving lectures from Edwards Lifesciences (Irvine, CA, USA). BS received institutional restricted research grants, honoraria for consulting, and refunds of travel expenses from Tensys Medical (San Diego, CA, USA). BS received honoraria for giving lectures and refunds of travel expenses from CNSystems Medizintechnik (Graz, Austria). BS received institutional restricted research grants from Retia Medical. BS received honoraria for giving lectures from Philips Medizin Systeme Böblingen (Böblingen, Germany). PH declared that he has no competing interests.
Figures
Similar articles
-
The rise of ward monitoring: opportunities and challenges for critical care specialists.Intensive Care Med. 2019 May;45(5):671-673. doi: 10.1007/s00134-018-5384-5. Epub 2018 Sep 27. Intensive Care Med. 2019. PMID: 30259073 No abstract available.
-
Feasibility of wireless continuous monitoring of vital signs without using alarms on a general surgical ward: A mixed methods study.PLoS One. 2022 Mar 14;17(3):e0265435. doi: 10.1371/journal.pone.0265435. eCollection 2022. PLoS One. 2022. PMID: 35286354 Free PMC article.
-
Implementation of a novel postoperative monitoring system using automated Modified Early Warning Scores (MEWS) incorporating end-tidal capnography.J Clin Monit Comput. 2017 Oct;31(5):1081-1092. doi: 10.1007/s10877-016-9943-4. Epub 2016 Oct 20. J Clin Monit Comput. 2017. PMID: 27766526
-
Postoperative ward monitoring - Why and what now?Best Pract Res Clin Anaesthesiol. 2019 Jun;33(2):229-245. doi: 10.1016/j.bpa.2019.06.005. Epub 2019 Jul 23. Best Pract Res Clin Anaesthesiol. 2019. PMID: 31582102 Review.
-
Improving detection of patient deterioration in the general hospital ward environment.Eur J Anaesthesiol. 2018 May;35(5):325-333. doi: 10.1097/EJA.0000000000000798. Eur J Anaesthesiol. 2018. PMID: 29474347 Free PMC article. Review.
Cited by
-
Advantage of Vital Sign Monitoring Using a Wireless Wearable Device for Predicting Septic Shock in Febrile Patients in the Emergency Department: A Machine Learning-Based Analysis.Sensors (Basel). 2022 Sep 17;22(18):7054. doi: 10.3390/s22187054. Sensors (Basel). 2022. PMID: 36146403 Free PMC article.
-
Clinical impact of vital sign abnormalities in patients admitted with acute exacerbation of chronic obstructive pulmonary disease: an observational study using continuous wireless monitoring.Intern Emerg Med. 2022 Sep;17(6):1689-1698. doi: 10.1007/s11739-022-02988-w. Epub 2022 May 20. Intern Emerg Med. 2022. PMID: 35593967
-
Early detection of deteriorating patients in general wards through continuous contactless vital signs monitoring.Front Med Technol. 2024 Aug 29;6:1436034. doi: 10.3389/fmedt.2024.1436034. eCollection 2024. Front Med Technol. 2024. PMID: 39328308 Free PMC article.
-
Early Warning Scores to Support Continuous Wireless Vital Sign Monitoring for Complication Prediction in Patients on Surgical Wards: Retrospective Observational Study.JMIR Perioper Med. 2023 Aug 30;6:e44483. doi: 10.2196/44483. JMIR Perioper Med. 2023. PMID: 37647104 Free PMC article.
-
Wireless wearables for postoperative surveillance on surgical wards: a survey of 1158 anaesthesiologists in Western Europe and the USA.BJA Open. 2022 Feb 23;1:100002. doi: 10.1016/j.bjao.2022.100002. eCollection 2022 Mar. BJA Open. 2022. PMID: 37588692 Free PMC article.
References
-
- Andersen LW, Berg KM, Chase M, Cocchi MN, Massaro J, Donnino MW. American Heart Association’s Get With The Guidelines-Resuscitation I: acute respiratory compromise on inpatient wards in the United States: incidence, outcomes, and factors associated with in-hospital mortality. Resuscitation. 2016;105:123–129. doi: 10.1016/j.resuscitation.2016.05.014. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
