

Blood Leukocyte Concentrations, FEV1 Decline, and Airflow Limitation. A 15-Year Longitudinal Study of World Trade Center-exposed Firefighters
- PMID: 29099614
- PMCID: PMC5802620
- DOI: 10.1513/AnnalsATS.201703-276OC
Blood Leukocyte Concentrations, FEV1 Decline, and Airflow Limitation. A 15-Year Longitudinal Study of World Trade Center-exposed Firefighters
Abstract
Rationale: Rescue/recovery work at the World Trade Center disaster site (WTC) caused a proximate decline in lung function in Fire Department of the City of New York firefighters. A subset of this cohort experienced an accelerated rate of lung function decline over 15 years of post-September 11, 2001 (9/11) follow-up.
Objectives: To determine if early postexposure blood leukocyte concentrations are biomarkers for subsequent FEV1 decline and incident airflow limitation.
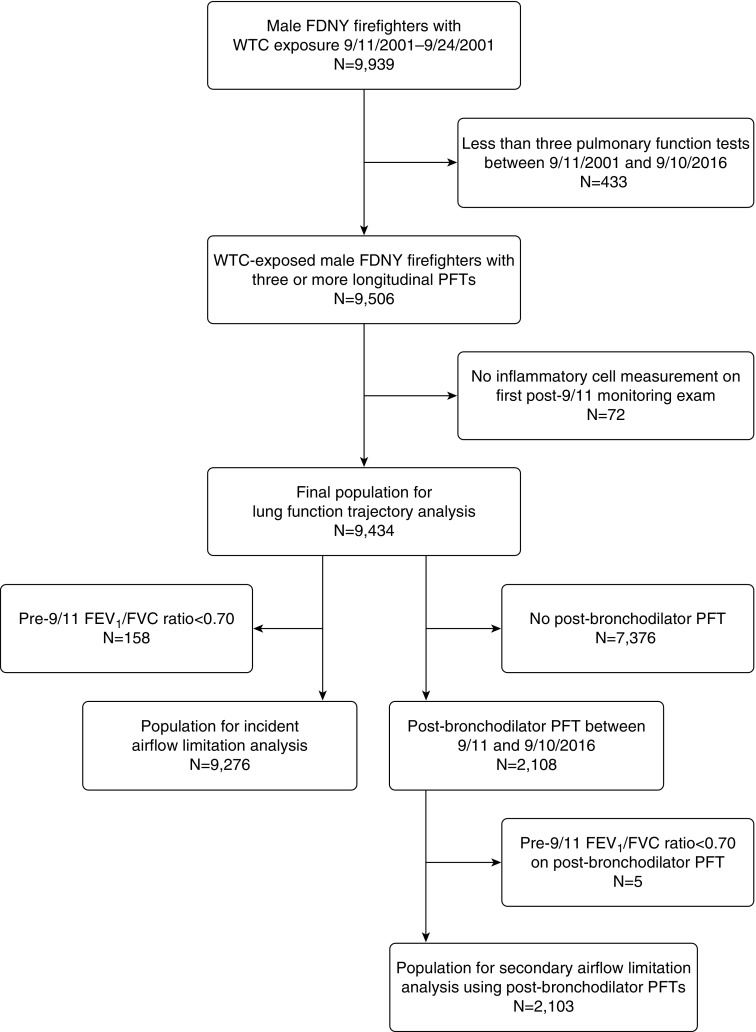
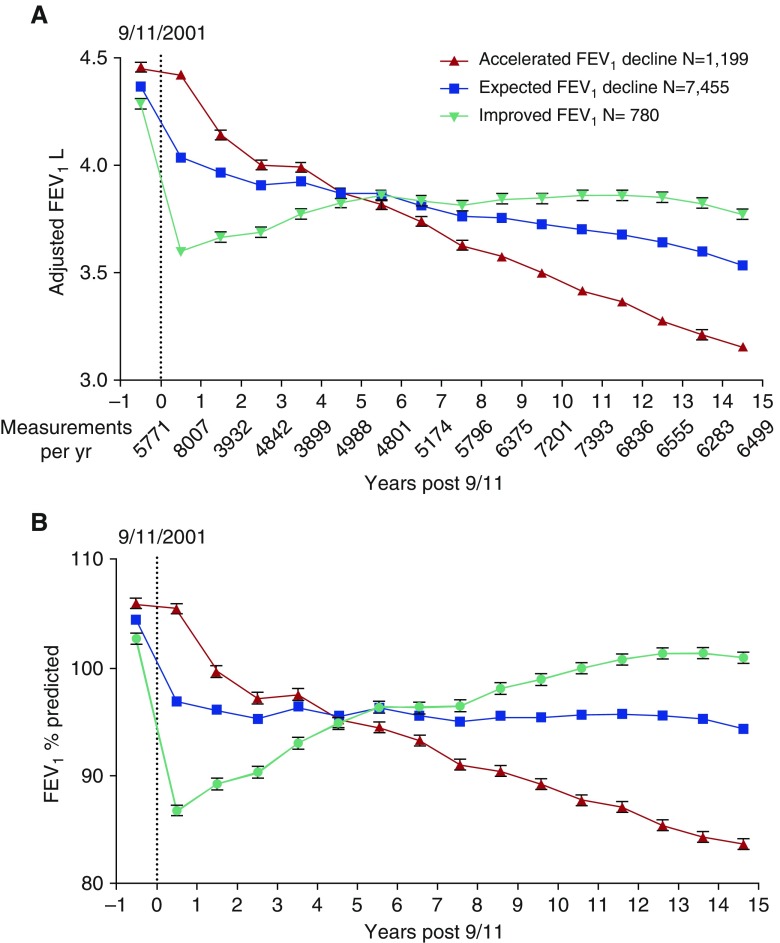
Methods: Individual rates of forced expiratory volume in 1 second (FEV1) change were calculated for 9,434 firefighters using 88,709 spirometric measurements taken between September 11, 2001, and September 10, 2016. We categorized FEV1 change rates into three trajectories: accelerated FEV1 decline (FEV1 loss >64 ml/yr), expected FEV1 decline (FEV1 loss between 0 and 64 ml/yr), and improved FEV1 (positive rate of change >0 ml/yr). Occurrence of FEV1/FVC less than 0.70 after 9/11 defined incident airflow limitation. Using regression models, we assessed associations of post-9/11 blood eosinophil and neutrophil concentrations with subsequent FEV1 decline and airflow limitation, adjusted for age, race, smoking, height, WTC exposure level, weight change, and baseline lung function.
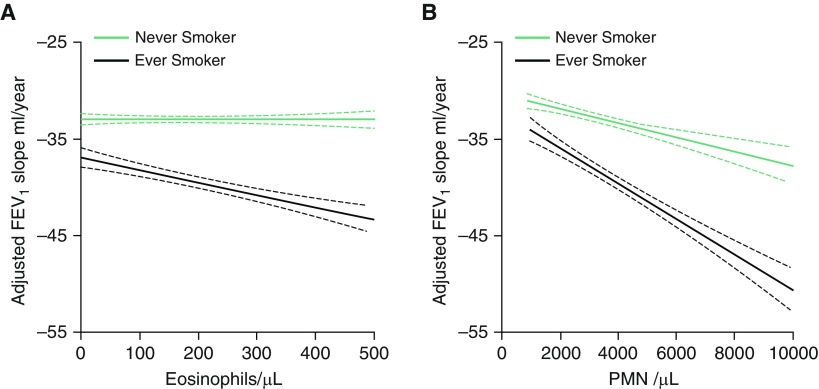
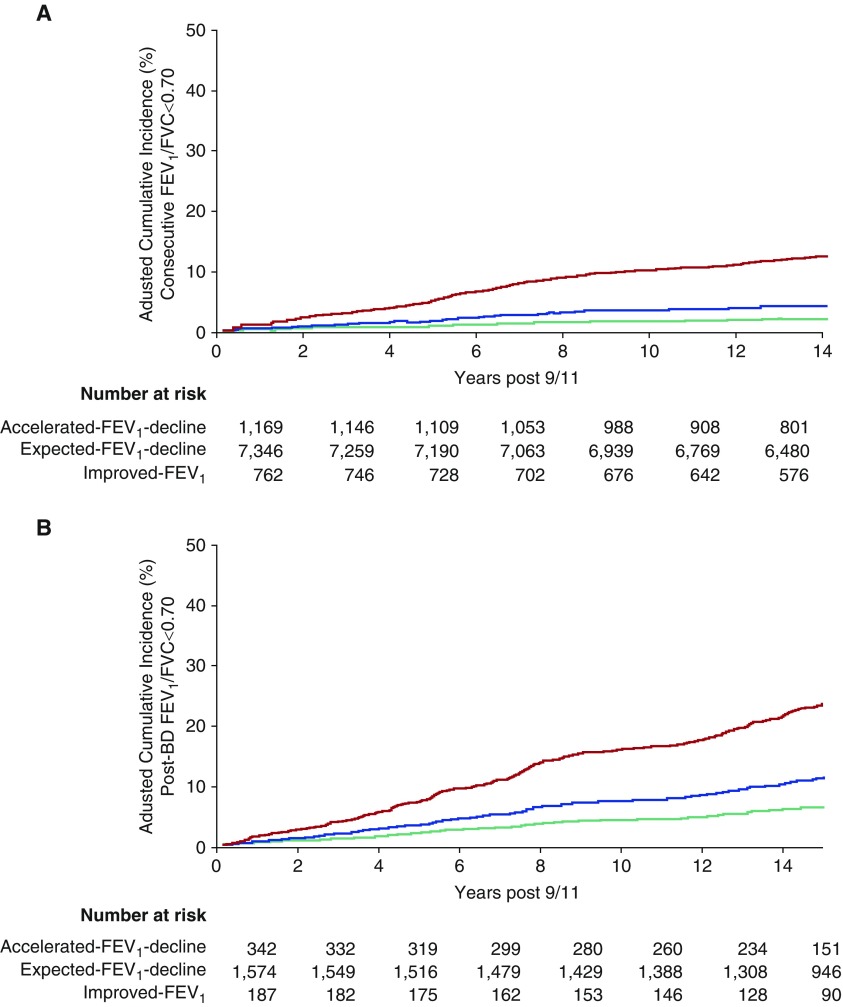
Results: Accelerated FEV1 decline occurred in 12.7% of participants (1,199 of 9,434), whereas post-9/11 FEV1 improvement occurred in 8.3% (780 of 9,434). Higher blood eosinophil and neutrophil concentrations were each associated with accelerated FEV1 decline after adjustment for covariates (odds ratio [OR], 1.10 per 100 eosinophils/μl; 95% confidence interval [CI], 1.05-1.15; and OR, 1.10 per 1,000 neutrophils/μl; 95% CI, 1.05-1.15, respectively). Multivariable-adjusted linear regression models showed that a higher blood neutrophil concentration was associated with a faster rate of FEV1 decline (1.14 ml/yr decline per 1,000 neutrophils/μl; 95% CI, 0.69-1.60 ml/yr; P < 0.001). Higher blood eosinophil concentrations were associated with a faster rate of FEV1 decline in ever-smokers (1.46 ml/yr decline per 100 eosinophils/μl; 95% CI, 0.65-2.26 ml/yr; P < 0.001) but not in never-smokers (P for interaction = 0.004). Higher eosinophil concentrations were also associated with incident airflow limitation (adjusted hazard ratio, 1.10 per 100 eosinophils/μl; 95% CI, 1.04-1.15). Compared with the expected FEV1 decline group, individuals experiencing accelerated FEV1 decline were more likely to have incident airflow limitation (adjusted OR, 4.12; 95% CI, 3.30-5.14).
Conclusions: Higher post-9/11 blood neutrophil and eosinophil concentrations were associated with subsequent accelerated FEV1 decline in WTC-exposed firefighters. Both higher blood eosinophil concentrations and accelerated FEV1 decline were associated with incident airflow limitation in WTC-exposed firefighters.
Keywords: eosinophils; longitudinal studies; lung injury; neutrophils; spirometry.
Figures
Comment in
-
Susceptibility to Inhalational Lung Injury: We Need More Than the FEV1.Ann Am Thorac Soc. 2018 Feb;15(2):156-157. doi: 10.1513/AnnalsATS.201711-870ED. Ann Am Thorac Soc. 2018. PMID: 29388819 No abstract available.
Similar articles
-
Predictors of Asthma/COPD Overlap in FDNY Firefighters With World Trade Center Dust Exposure: A Longitudinal Study.Chest. 2018 Dec;154(6):1301-1310. doi: 10.1016/j.chest.2018.07.002. Epub 2018 Jul 17. Chest. 2018. PMID: 30028968 Free PMC article.
-
Blood Eosinophils and World Trade Center Exposure Predict Surgery in Chronic Rhinosinusitis. A 13.5-Year Longitudinal Study.Ann Am Thorac Soc. 2016 Aug;13(8):1253-61. doi: 10.1513/AnnalsATS.201511-742OC. Ann Am Thorac Soc. 2016. PMID: 27096198 Free PMC article.
-
Serum Th-2 cytokines and FEV1 decline in WTC-exposed firefighters: A 19-year longitudinal study.Am J Ind Med. 2021 Oct;64(10):845-852. doi: 10.1002/ajim.23276. Epub 2021 Jul 20. Am J Ind Med. 2021. PMID: 34288008 Free PMC article.
-
Biomarkers of World Trade Center Particulate Matter Exposure: Physiology of Distal Airway and Blood Biomarkers that Predict FEV₁ Decline.Semin Respir Crit Care Med. 2015 Jun;36(3):323-33. doi: 10.1055/s-0035-1547349. Epub 2015 May 29. Semin Respir Crit Care Med. 2015. PMID: 26024341 Free PMC article. Review.
-
Twenty-Year Reflection on the Impact of World Trade Center Exposure on Pulmonary Outcomes in Fire Department of the City of New York (FDNY) Rescue and Recovery Workers.Lung. 2021 Dec;199(6):569-578. doi: 10.1007/s00408-021-00493-z. Epub 2021 Nov 11. Lung. 2021. PMID: 34766209 Free PMC article. Review.
Cited by
-
Association of Lung Function Decline with All-Cause and Cancer-Cause Mortality after World Trade Center Dust Exposure.Ann Am Thorac Soc. 2023 Aug;20(8):1136-1143. doi: 10.1513/AnnalsATS.202212-1011OC. Ann Am Thorac Soc. 2023. PMID: 36961515 Free PMC article.
-
Biomarkers of Airway Disease, Barrett's and Underdiagnosed Reflux Noninvasively (BAD-BURN): a Case-Control Observational Study Protocol.Res Sq [Preprint]. 2024 May 15:rs.3.rs-4355584. doi: 10.21203/rs.3.rs-4355584/v1. Res Sq. 2024. Update in: BMC Gastroenterol. 2024 Aug 9;24(1):255. doi: 10.1186/s12876-024-03294-9 PMID: 38798396 Free PMC article. Updated. Preprint.
-
Long-term Cardiovascular Disease Risk Among Firefighters After the World Trade Center Disaster.JAMA Netw Open. 2019 Sep 4;2(9):e199775. doi: 10.1001/jamanetworkopen.2019.9775. JAMA Netw Open. 2019. PMID: 31490535 Free PMC article.
-
Dyspnea and Inhaled Corticosteroid and Long-acting β-Agonist Therapy in an Occupational Cohort: A Longitudinal Study.Ann Am Thorac Soc. 2020 Jun;17(6):770-773. doi: 10.1513/AnnalsATS.201910-794RL. Ann Am Thorac Soc. 2020. PMID: 32068437 Free PMC article. No abstract available.
-
COPD in Firefighters: A Specific Event-Related Condition Rather than a Common Occupational Respiratory Disorder.Medicina (Kaunas). 2022 Feb 5;58(2):239. doi: 10.3390/medicina58020239. Medicina (Kaunas). 2022. PMID: 35208563 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
