

Trends and advances in tumor immunology and lung cancer immunotherapy
- PMID: 27686848
- PMCID: PMC5043622
- DOI: 10.1186/s13046-016-0439-3
Trends and advances in tumor immunology and lung cancer immunotherapy
Abstract
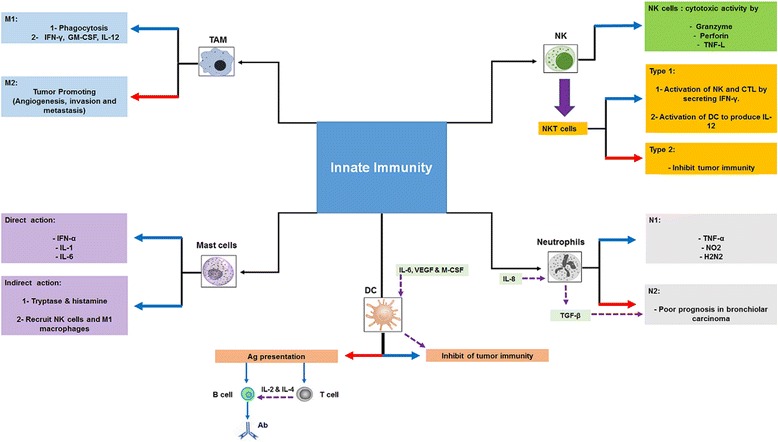
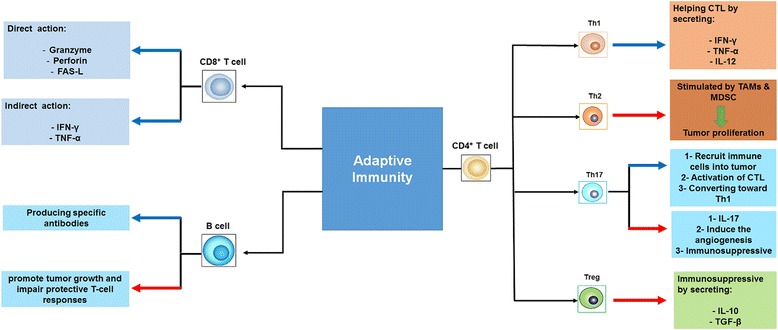
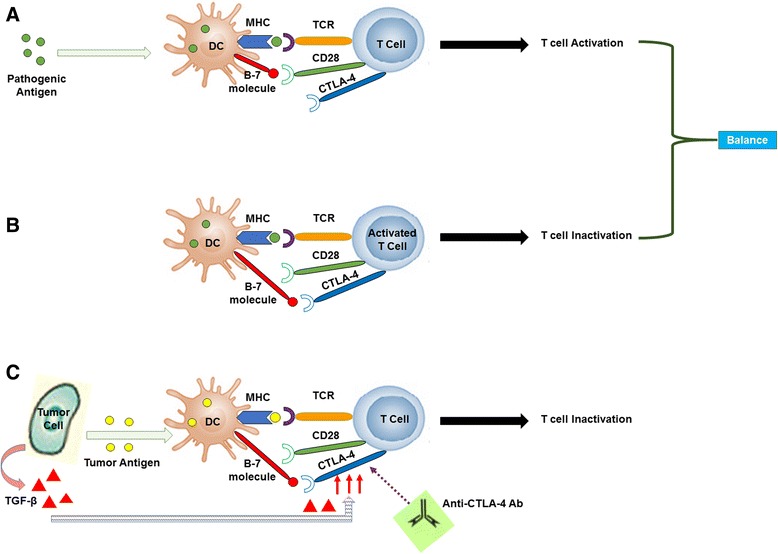
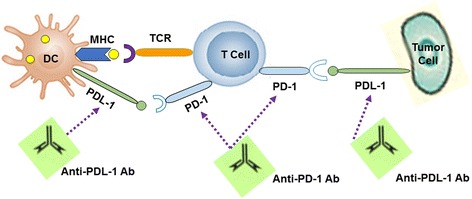
Among several types of tumor, lung cancer is considered one of the most fatal and still the main cause of cancer-related deaths. Although chemotherapeutic agents can improve survival and quality of life compared with symptomatic treatment, cancers usually still progress after chemotherapy and are often aggravated by serious side effects. In the last few years there has been a growing interest in immunotherapy for lung cancer based on promising preliminary results in achieving meaningful and durable treatments responses with minimal manageable toxicity. This article is divided into two parts, the first part discusses the role of human immune system in controlling and eradicating cancer and the mechanisms of immune response evasion by tumor. The second part reviews the recent progress made in immunotherapy for lung cancer with results from trials evaluating therapeutic vaccines in addition to immune checkpoint blockade, specifically cytotoxic T lymphocyte associated protein 4, programmed death receptor 1 pathway, using monoclonal antibodies.
Keywords: Cancer vaccines; Clinical trials; Immune checkpoint inhibitors; Immunotherapy; Lung cancer; Tumor immunology.
Figures
Similar articles
-
The effectiveness of school-based family asthma educational programs on the quality of life and number of asthma exacerbations of children aged five to 18 years diagnosed with asthma: a systematic review protocol.JBI Database System Rev Implement Rep. 2015 Oct;13(10):69-81. doi: 10.11124/jbisrir-2015-2335. JBI Database System Rev Implement Rep. 2015. PMID: 26571284
-
Comparison of Two Modern Survival Prediction Tools, SORG-MLA and METSSS, in Patients With Symptomatic Long-bone Metastases Who Underwent Local Treatment With Surgery Followed by Radiotherapy and With Radiotherapy Alone.Clin Orthop Relat Res. 2024 Dec 1;482(12):2193-2208. doi: 10.1097/CORR.0000000000003185. Epub 2024 Jul 23. Clin Orthop Relat Res. 2024. PMID: 39051924
-
Improving PD-1 blockade plus chemotherapy for complete remission of lung cancer by nanoPDLIM2.Elife. 2024 Dec 24;12:RP89638. doi: 10.7554/eLife.89638. Elife. 2024. PMID: 39718207 Free PMC article.
-
Depressing time: Waiting, melancholia, and the psychoanalytic practice of care.In: Kirtsoglou E, Simpson B, editors. The Time of Anthropology: Studies of Contemporary Chronopolitics. Abingdon: Routledge; 2020. Chapter 5. In: Kirtsoglou E, Simpson B, editors. The Time of Anthropology: Studies of Contemporary Chronopolitics. Abingdon: Routledge; 2020. Chapter 5. PMID: 36137063 Free Books & Documents. Review.
-
Immune checkpoint inhibitors plus platinum-based chemotherapy compared to platinum-based chemotherapy with or without bevacizumab for first-line treatment of older people with advanced non-small cell lung cancer.Cochrane Database Syst Rev. 2024 Aug 13;8(8):CD015495. doi: 10.1002/14651858.CD015495. Cochrane Database Syst Rev. 2024. PMID: 39136258 Review.
Cited by
-
A study on fractional tumor-immune interaction model related to lung cancer via generalized Laguerre polynomials.BMC Med Res Methodol. 2023 Aug 21;23(1):189. doi: 10.1186/s12874-023-02006-3. BMC Med Res Methodol. 2023. PMID: 37605131 Free PMC article.
-
The effects of postoperative targeted immunotherapy on peripheral blood cytokines and immune cell profile in lung cancer patients.Front Oncol. 2024 Jun 5;14:1342624. doi: 10.3389/fonc.2024.1342624. eCollection 2024. Front Oncol. 2024. PMID: 38903721 Free PMC article.
-
Integrated analysis of single-cell and Bulk RNA sequencing reveals a malignancy-related signature in lung adenocarcinoma.Front Oncol. 2023 Jun 23;13:1198746. doi: 10.3389/fonc.2023.1198746. eCollection 2023. Front Oncol. 2023. PMID: 37427142 Free PMC article.
-
Functional Engagement of the PD-1/PD-L1 Complex But Not PD-L1 Expression Is Highly Predictive of Patient Response to Immunotherapy in Non-Small-Cell Lung Cancer.J Clin Oncol. 2023 May 10;41(14):2561-2570. doi: 10.1200/JCO.22.01748. Epub 2023 Feb 23. J Clin Oncol. 2023. PMID: 36821809 Free PMC article.
-
Budding uninhibited by benzimidazoles 1 overexpression is associated with poor prognosis and malignant phenotype: A promising therapeutic target for lung adenocarcinoma.Thorac Cancer. 2023 Apr;14(10):893-912. doi: 10.1111/1759-7714.14822. Epub 2023 Feb 24. Thorac Cancer. 2023. PMID: 36825773 Free PMC article.
References
-
- Schuster M, Nechansky A, Kircheis R. Cancer immunotherapy. Biogeosciences. 2006;1(2):138–47. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
