

Interrater reliability of the Wolf Motor Function Test-Functional Ability Scale: why it matters
- PMID: 25323459
- PMCID: PMC4400190
- DOI: 10.1177/1545968314553030
Interrater reliability of the Wolf Motor Function Test-Functional Ability Scale: why it matters
Abstract
Background: One important objective for clinical trialists in rehabilitation is determining efficacy of interventions to enhance motor behavior. In part, limitation in the precision of measurement presents a challenge. The few valid, low-cost observational tools available to assess motor behavior cannot escape the variability inherent in test administration and scoring. This is especially true when there are multiple evaluators and raters, as in the case of multisite randomized controlled trials (RCTs). One way to enhance reliability and reduce variability is to implement rigorous quality control (QC) procedures.
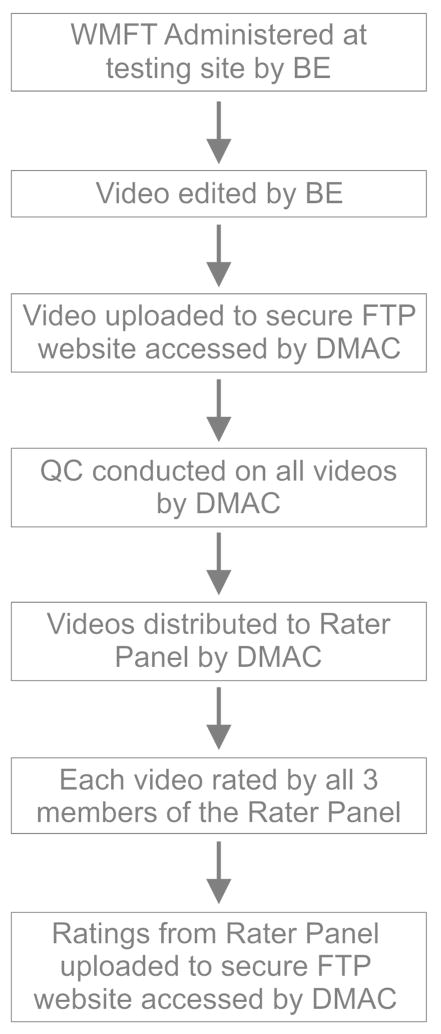
Objective: This article describes a systematic QC process used to refine the administration and scoring procedures for the Wolf Motor Function Test (WMFT)-Functional Ability Scale (FAS).
Methods: The QC process, a systematic focus-group collaboration, was developed and used for a phase III RCT, which enlisted multiple evaluators and an experienced WMFT-FAS rater panel.
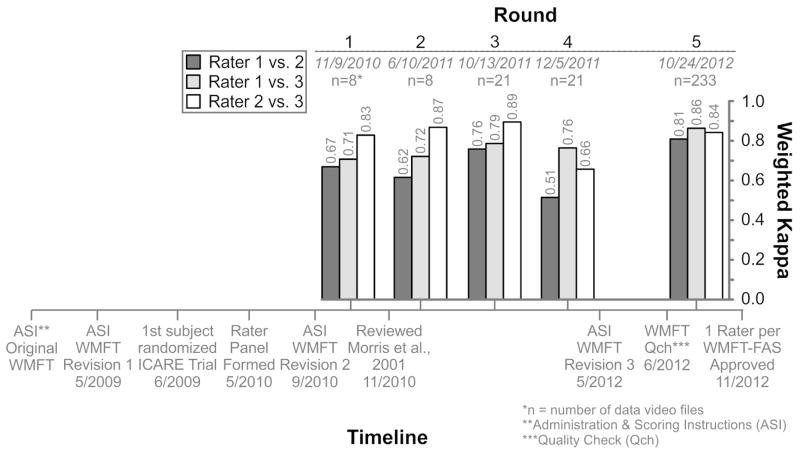
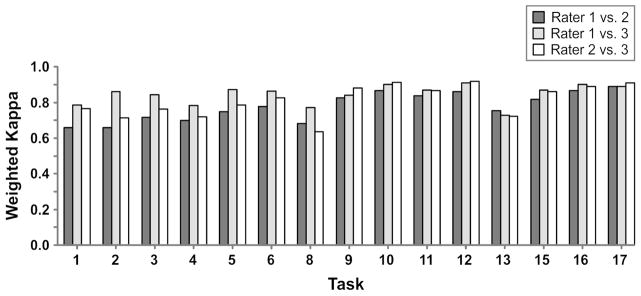
Results: After 3 staged refinements to the administration and scoring instructions, we achieved a sufficiently high interrater reliability (weighted κ = 0.8).
Conclusions and implications: A systematic focus-group process was shown to be an effective method to improve reliability of observational assessment tools for motor behavior in neurorehabilitation. A reduction in noise-related variability in performance assessments will increase power and potentially lower the number needed to treat. Improved precision of measurement can lead to more cost-effective and efficient clinical trials. Finally, we suggest that improved precision in measures of motor behavior may provide more insight into recovery mechanisms than a single measure of movement time alone.
Keywords: assessment; impairment; motor control; observational; quality; stroke.
© The Author(s) 2014.
Figures
Similar articles
-
Inter-rater reliability, sensitivity to change and responsiveness of the orthopaedic Wolf-Motor-Function-Test as functional capacity measure before and after rehabilitation in patients with proximal humeral fractures.BMC Musculoskelet Disord. 2019 Jul 6;20(1):315. doi: 10.1186/s12891-019-2691-0. BMC Musculoskelet Disord. 2019. PMID: 31279331 Free PMC article. Clinical Trial.
-
The future of Cochrane Neonatal.Early Hum Dev. 2020 Nov;150:105191. doi: 10.1016/j.earlhumdev.2020.105191. Epub 2020 Sep 12. Early Hum Dev. 2020. PMID: 33036834
-
The reliability of the wolf motor function test for assessing upper extremity function after stroke.Arch Phys Med Rehabil. 2001 Jun;82(6):750-5. doi: 10.1053/apmr.2001.23183. Arch Phys Med Rehabil. 2001. PMID: 11387578
-
Review of the randomized clinical stroke rehabilitation trials in 2009.Med Sci Monit. 2011 Feb;17(2):RA25-43. doi: 10.12659/msm.881382. Med Sci Monit. 2011. PMID: 21278702 Free PMC article. Review.
-
Evaluation of functional outcome measures for the hemiparetic upper limb: a systematic review.J Rehabil Med. 2008 Nov;40(10):787-95. doi: 10.2340/16501977-0276. J Rehabil Med. 2008. PMID: 19242614 Review.
Cited by
-
A Reaching Performance Scale for 2 Wolf Motor Function Test Items.Arch Phys Med Rehabil. 2020 Nov;101(11):2015-2026. doi: 10.1016/j.apmr.2020.05.003. Epub 2020 May 17. Arch Phys Med Rehabil. 2020. PMID: 32433993 Free PMC article.
-
Improving patient outcomes in acute and subacute stroke using a wearable device-assisted rehabilitation system: a randomized controlled trial.J Int Med Res. 2024 Oct;52(10):3000605241281425. doi: 10.1177/03000605241281425. J Int Med Res. 2024. PMID: 39387211 Free PMC article. Clinical Trial.
-
Design of a Data Glove for Assessment of Hand Performance Using Supervised Machine Learning.Sensors (Basel). 2021 Oct 20;21(21):6948. doi: 10.3390/s21216948. Sensors (Basel). 2021. PMID: 34770255 Free PMC article.
-
Predicting and Monitoring Upper-Limb Rehabilitation Outcomes Using Clinical and Wearable Sensor Data in Brain Injury Survivors.IEEE Trans Biomed Eng. 2021 Jun;68(6):1871-1881. doi: 10.1109/TBME.2020.3027853. Epub 2021 May 21. IEEE Trans Biomed Eng. 2021. PMID: 32997621 Free PMC article.
-
Effects of Real-Time (Sonification) and Rhythmic Auditory Stimuli on Recovering Arm Function Post Stroke: A Systematic Review and Meta-Analysis.Front Neurol. 2018 Jul 13;9:488. doi: 10.3389/fneur.2018.00488. eCollection 2018. Front Neurol. 2018. PMID: 30057563 Free PMC article.
References
-
- Kitago T, Liang J, Huang VS, et al. Improvement after constraint-induced movement therapy: recovery of normal motor control or task-specific compensation? Neurorehabil Neural Repair. 2013;27:99–109. - PubMed
-
- van Kordelaar J, van Wegan EE, Kwakkel G. The impact of time on quality of motor control of the paretic upper limb after stroke. Arch Phys Med Rehabil. 2014;95:338–44. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
