

Using perceptive computing in multiple sclerosis - the Short Maximum Speed Walk test
- PMID: 24886525
- PMCID: PMC4041903
- DOI: 10.1186/1743-0003-11-89
Using perceptive computing in multiple sclerosis - the Short Maximum Speed Walk test
Abstract
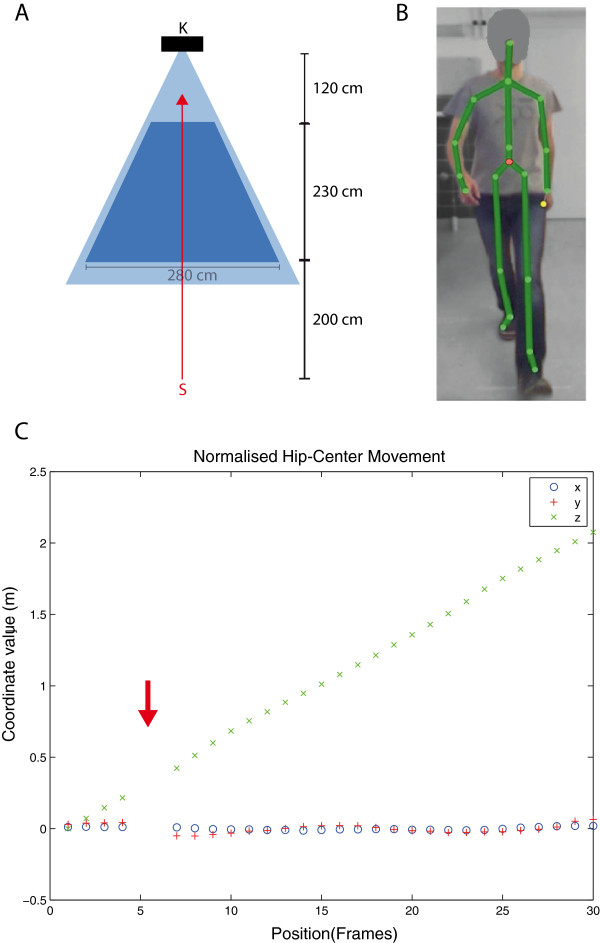
Background: We investigated the applicability and feasibility of perceptive computing assisted gait analysis in multiple sclerosis (MS) patients using Microsoft Kinect™. To detect the maximum walking speed and the degree of spatial sway, we established a computerized and observer-independent measure, which we named Short Maximum Speed Walk (SMSW), and compared it to established clinical measures of gait disability in MS, namely the Expanded Disability Status Scale (EDSS) and the Timed 25-Foot Walk (T25FW).
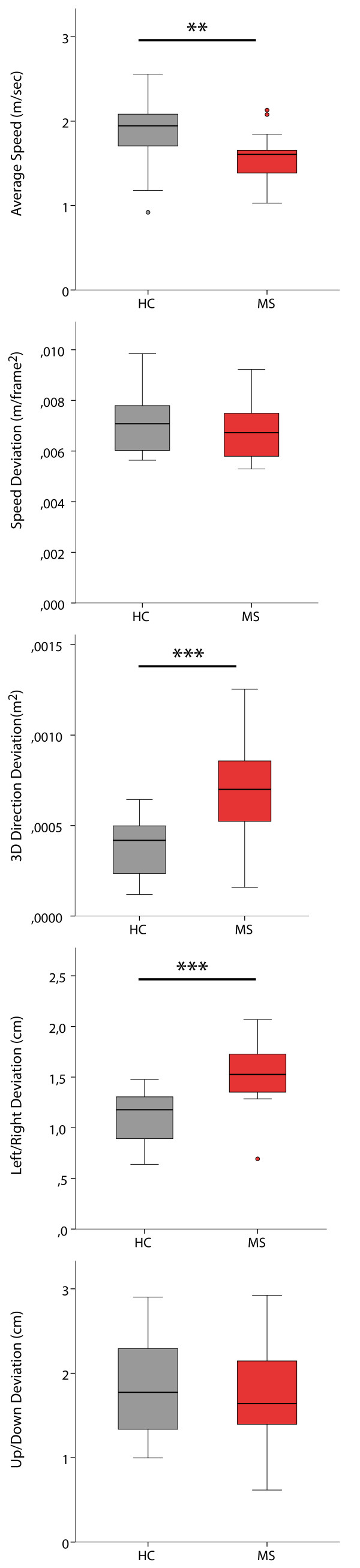
Methods: Cross-sectional study of 22 MS patients (age mean ± SD 43 ± 9 years, 13 female) and 22 age and gender matched healthy control subjects (HC) (age 37 ± 11 years, 13 female). The disability level of each MS patient was graded using the EDSS (median 3.0, range 0.0-6.0). All subjects then performed the SMSW and the Timed 25-Foot Walk (T25FW). The SMSW comprised five gait parameters, which together assessed average walking speed and gait stability in different dimensions (left/right, up/down and 3D deviation).
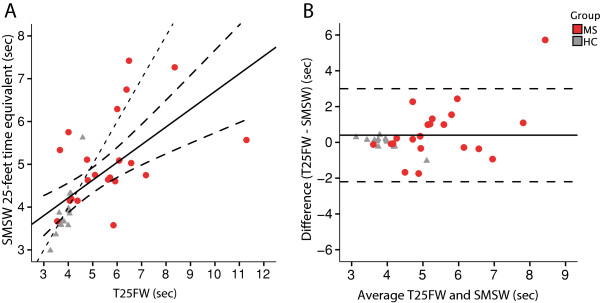
Results: SMSW average walking speed was slower in MS patients (1.6 ± 0.3 m/sec) than in HC (1.8 ± 0.4 m/sec) (p = 0.005) and correlated well with EDSS (Spearman's Rho 0.676, p < 0.001). Furthermore, SMSW revealed higher left/right deviation in MS patients compared to HC. SMSW showed high recognition quality and retest-reliability (covariance 0.13 m/sec, ICC 0.965, p < 0.001). There was a significant correlation between SMSW average walking speed and T25FW (Pearson's R = -0.447, p = 0.042).
Conclusion: Our data suggest that ambulation tests using Microsoft Kinect™ are feasible, well tolerated and can detect clinical gait disturbances in patients with MS. The retest-reliability was on par with the T25FW.
Figures
Similar articles
-
Maximum walking speed in multiple sclerosis assessed with visual perceptive computing.PLoS One. 2017 Dec 15;12(12):e0189281. doi: 10.1371/journal.pone.0189281. eCollection 2017. PLoS One. 2017. PMID: 29244874 Free PMC article.
-
Japanese translation and validation of the 12-item Multiple Sclerosis Walking Scale version 2.Mult Scler Relat Disord. 2024 Sep;89:105768. doi: 10.1016/j.msard.2024.105768. Epub 2024 Jul 11. Mult Scler Relat Disord. 2024. PMID: 39003823
-
The six spot step test: a new measurement for walking ability in multiple sclerosis.Mult Scler. 2006 Aug;12(4):495-500. doi: 10.1191/1352458506ms1293oa. Mult Scler. 2006. PMID: 16900764 Clinical Trial.
-
Timed 25-foot walk: direct evidence that improving 20% or greater is clinically meaningful in MS.Neurology. 2013 Apr 16;80(16):1509-17. doi: 10.1212/WNL.0b013e31828cf7f3. Epub 2013 Mar 27. Neurology. 2013. PMID: 23535489 Review.
-
Assessing walking disability in multiple sclerosis.Mult Scler. 2012 Jul;18(7):914-24. doi: 10.1177/1352458512444498. Epub 2012 Apr 24. Mult Scler. 2012. PMID: 22740603 Review.
Cited by
-
Kinematic synergies show good consistency when extracted with a low-cost markerless device and a marker-based motion tracking system.Heliyon. 2024 May 28;10(11):e32042. doi: 10.1016/j.heliyon.2024.e32042. eCollection 2024 Jun 15. Heliyon. 2024. PMID: 38882310 Free PMC article.
-
Digital Motor Biomarkers of Cerebellar Ataxia Using an RGB-Depth Camera-Based Motion Analysis System.Cerebellum. 2024 Jun;23(3):1031-1041. doi: 10.1007/s12311-023-01604-7. Epub 2023 Sep 18. Cerebellum. 2024. PMID: 37721679
-
RGB-Depth Camera-Based Assessment of Motor Capacity: Normative Data for Six Standardized Motor Tasks.Int J Environ Res Public Health. 2022 Dec 17;19(24):16989. doi: 10.3390/ijerph192416989. Int J Environ Res Public Health. 2022. PMID: 36554871 Free PMC article.
-
Healthcare applications of single camera markerless motion capture: a scoping review.PeerJ. 2022 May 26;10:e13517. doi: 10.7717/peerj.13517. eCollection 2022. PeerJ. 2022. PMID: 35642200 Free PMC article. Review.
-
Proposal for Post Hoc Quality Control in Instrumented Motion Analysis Using Markerless Motion Capture: Development and Usability Study.JMIR Hum Factors. 2022 Apr 1;9(2):e26825. doi: 10.2196/26825. JMIR Hum Factors. 2022. PMID: 35363150 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
